Case 11. Progressive communication difficulties
Where is the lesion?
The chief symptom is of progressive language dysfunction (dysphasia).
Dysphasia is not a speech issue but a language one – the patient also has difficulty with writing, so it isn't just oral word output, and likewise there are some issues with comprehension.
Speech problems are distinct from this (dysarthria, dysphonia) - i.e. they are issues with the actual production of oral word output. The distinction is fundamental - and there is a reason an entire profession exists termed Speech and Language Therapy!
Some people have problems in both, for example large strokes affecting both the language centres in the brain as well as the motor parts involved in speech mechanics. However, there are many examples of a problem in only one. For example this patient, who has dysphasia. Another example would be someone who cannot produce speech, yet has intact language function and can still write or communicate through blinking - examples of this include people with neuromuscular disorders, or those with an endotracheal tube who are conscious.
In addition she has a right homonymous quadrantanopia identified on examination. She had no symptoms from this, and this is often the case with post-chiasmatic visual field problems - patients often are not aware of the defect and do not complain of visual loss, but instead may bump into objects they don't notice - or it is found on examination alone.
Combined dysphasia and quadrantanopia localises to the brain, and we know the issue is in the left hemisphere for two reasons:
Can we localise this further?
1. DysphasiaThe pattern is of a mixed dysphasia. There is an expressive element, with word-finding difficulties and paraphasic errors. There is also a receptive one, with impaired verbal understanding at points (including multi-step commands) and lack of recognition of the errors she is making - her partner instead noticed those.
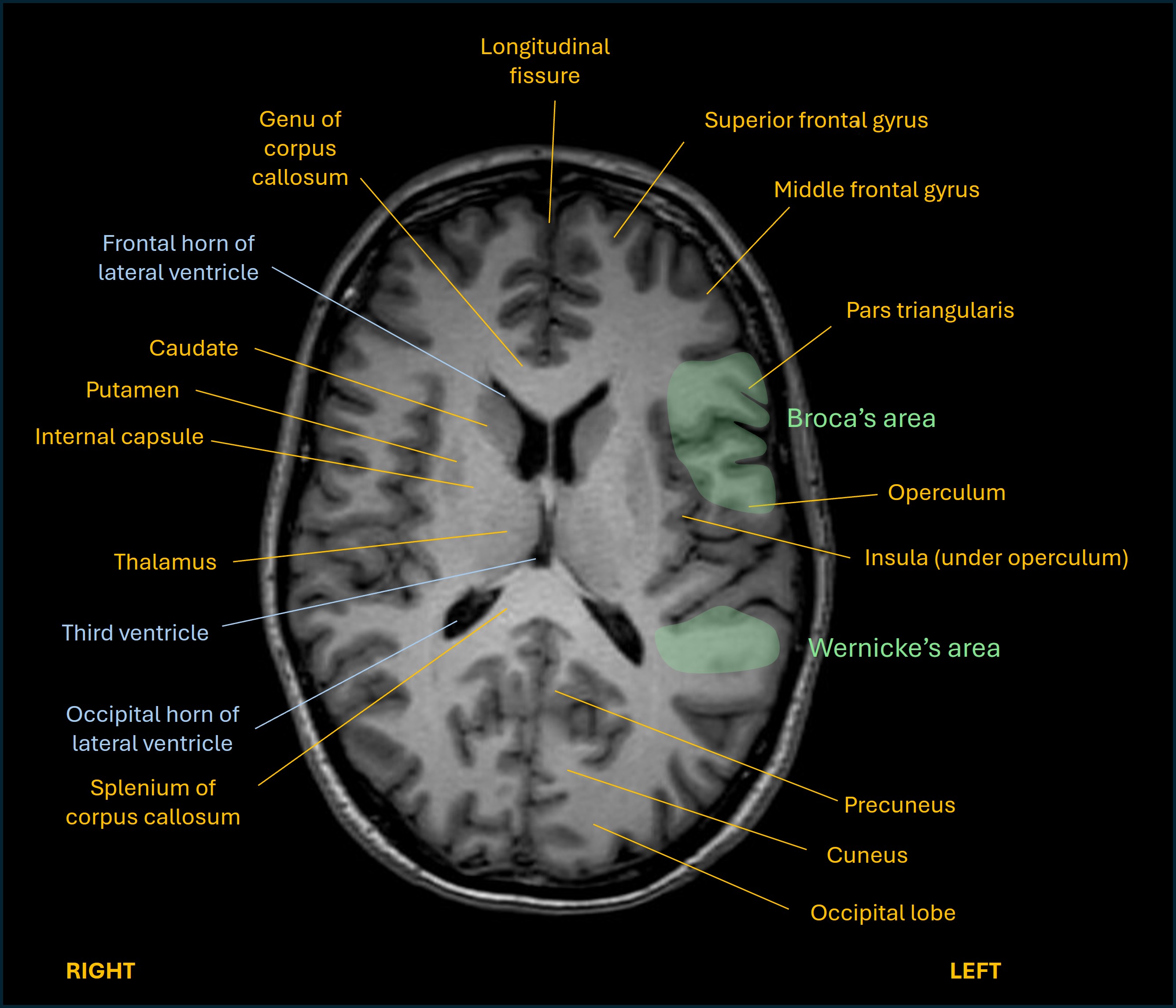
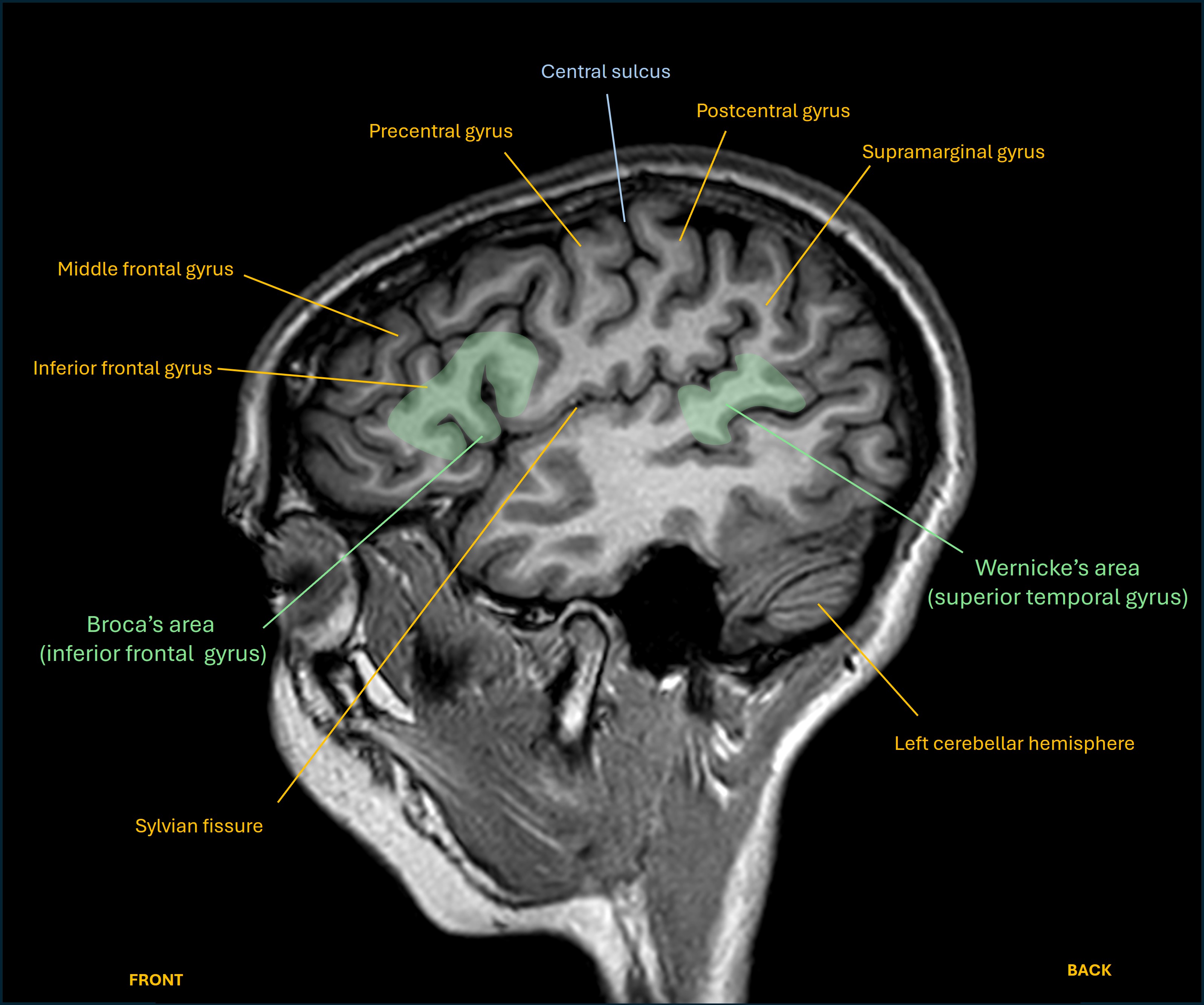
This mixed pattern suggests a lesion somewhere overlapping the left frontal lobe (expressive) and temporal lobe (receptive) language centres, which must involve the subcortical white matter structures connecting these. The fact that the severity is only moderate also fits this - often a lesion centred in the language centre itself produces more profound dysphasia. (Of note, the term aphasia is often used interchangeably with dysphasia - but should really mean a more profound language deficit, or even complete loss of language functions.)
Her dysphasia pattern is different from the two well-known ‘pure’ expressive and receptive forms:
In practice, patients often have a mixed pattern, and the severity may be worse for one element (e.g. severe expressive with minor receptive difficulties).
 2. Quadrantanopia
2. Quadrantanopia
The right homonymous inferior quadrantanopia suggests involvement of the left superior optic radiation in the parietal and/or occipital lobe. The optic radiation does not extend to the parietal cortex – it is a subcortical white matter tract.
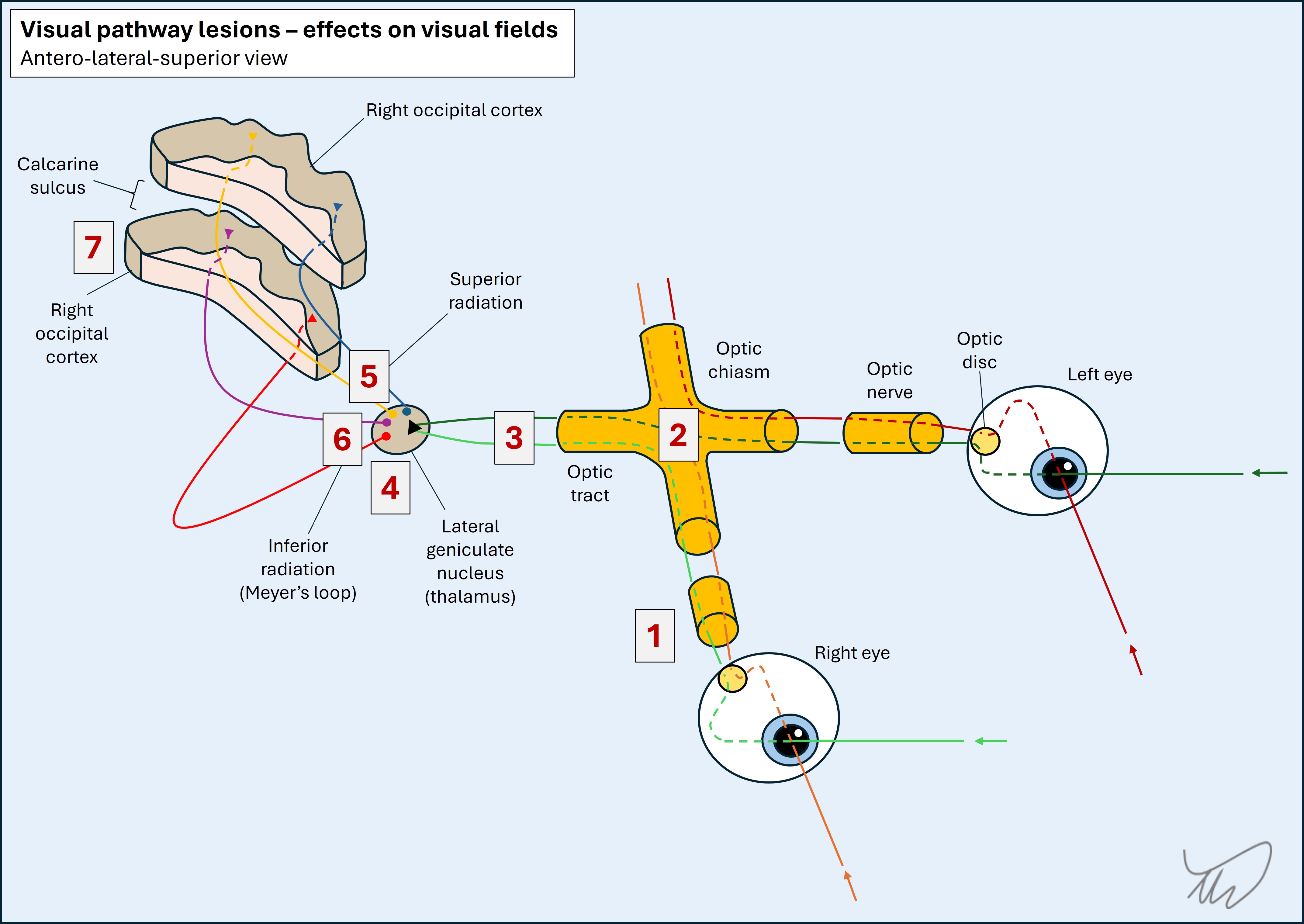
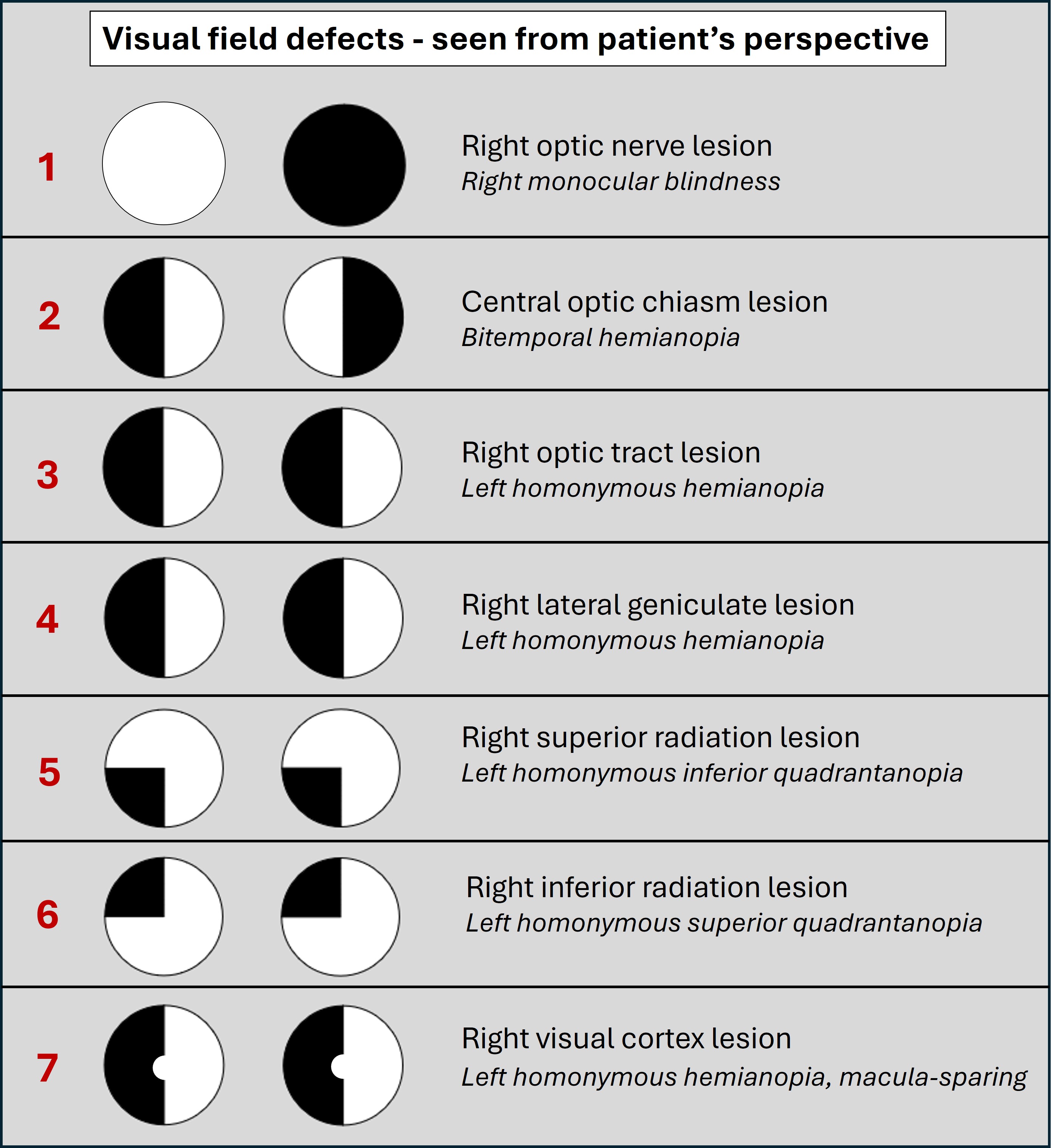
Note - we have reviewed the visual field pathways in more depth in an earlier case; for a detailed recap of this, consider revisiting the section - Case 8 - where is the lesion?
SummaryThis lesion must be left hemispheric, involving subcortical tracts including the superior optic radiation and the connections between the frontal and temporal language centres. The left parietal lobe subcortical area seems likely.
What is the lesion?